

When it comes to problems with TMJ Disorder, it turns out that kids have problems at almost twice the rate of adults.
Nearly 1 of 4 children ages kindergarten to 5th grade, report TMJ/D symptoms a new study reports in the February 2016 journal of the American Dental Association. This study of children found that girls had about 4% higher incidence of symptoms surveyed than boys.
It coincides with a 2014 study that found 25% of 12-14 year olds have TMJ-related pain. That’s twice the rate of adults who suffer TMJ problems at about the rate of 5-12% of the population, according to the National Institute of Dental and Craniofacial research in 2014.
The TMJ, or Temporomandibular Joint (the jaw joint by our ear), allows the mouth to move. It is one of the most complex joints in the body, having two simultaneous movements – rotating and sliding. The mandible (our lower jaw) has two independent joints (TMJ) at either end. Movement of one joint causes movement of the other, for good or bad. It’s very susceptible to damage or wear and tear injury.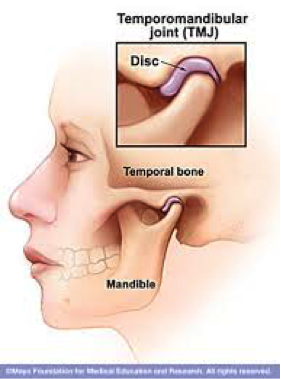
What should parent’s and dentists look for?
This study asked over 8000 children three specific questions:
- Do you have pain in your face when you eat?
- Do you have pain when you open your mouth wide?
- Do you hear “clicking” when you open your mouth?
As a parent you can ask your kids about this, especially if they seem irritable or unable to eat, or if they start grinding their teeth at night. When I practiced general dentistry (before specializing in TMJ and sleep apnea) I always evaluated the TMJ and neck of children, and almost weekly treated at least one child experiencing pain. While growing, intervention can sometimes be easier than in adults or adolescents who have stopped growing. A big contributing factor in future TMJ liability in growing children are airway and breathing problems. It interferes with development of the upper and lower jaws, leading to abnormal alignment of the TMJ, irregular swallowing patterns, and malocclusion. I’ve written earlier about this.
This study also ruled out poor dental health being a factor in these children reporting facial pain and TMJ clicking. The population was almost an equal 50/50 split between boys and girls too.
All dentists, pediatricians, and other health care professionals should be screening everyone for TMJ problems at every visit. The problem is, we weren’t taught anything about it in dental school and still aren’t today. Nor are other professions. The official ADA stance remains that TMJ is a self-limiting condition that should be treated as a stress-related symptom. That’s a small part, but TMJD (temporomandibular Joint Disorders) is an orthopedic disorder that responds well to orthopedic principles meaning – distract or unload the joint, align, and re-train functional movement. That’s what I do with TMJ orthotics. Dental “splints” or night guards do not typically treat TMJD.
The medical profession also adopts Dentistry’s official opinion and typically medicates women with antidepressants, anti-anxiety medication or migraine meds when they reach out for help with Orofacial Pain.
As noted in my last blog post, my preferred method of treatment is to start with joint traction/decompression with orthotics, use physical medicine to restore mobility in the neck if needed and then re-evaluate whether there is non-responding muscle pain that might benefit from some other form of pain relief.
Contact our office today to schedule an evaluation.

